Redlining and housing discrimination have had a profound legacy on the urban fabric of many cities. Areas that were historically redlined have been shown to have more dilapidated structures, lower tree canopy coverage, a higher density of multi-family buildings, and other differences relative to the built environment of non-redlined areas. We know that in Louisville, in particular, tree canopy coverage is lower in redlined neighborhoods. Tree canopy coverage has a plethora of positive effects on human health by lowering the urban heat island effect, improving mental health, lowering blood pressure, and more. Decades of underinvestment can also make these areas less walkable and lack important amenities such as healthcare facilities.
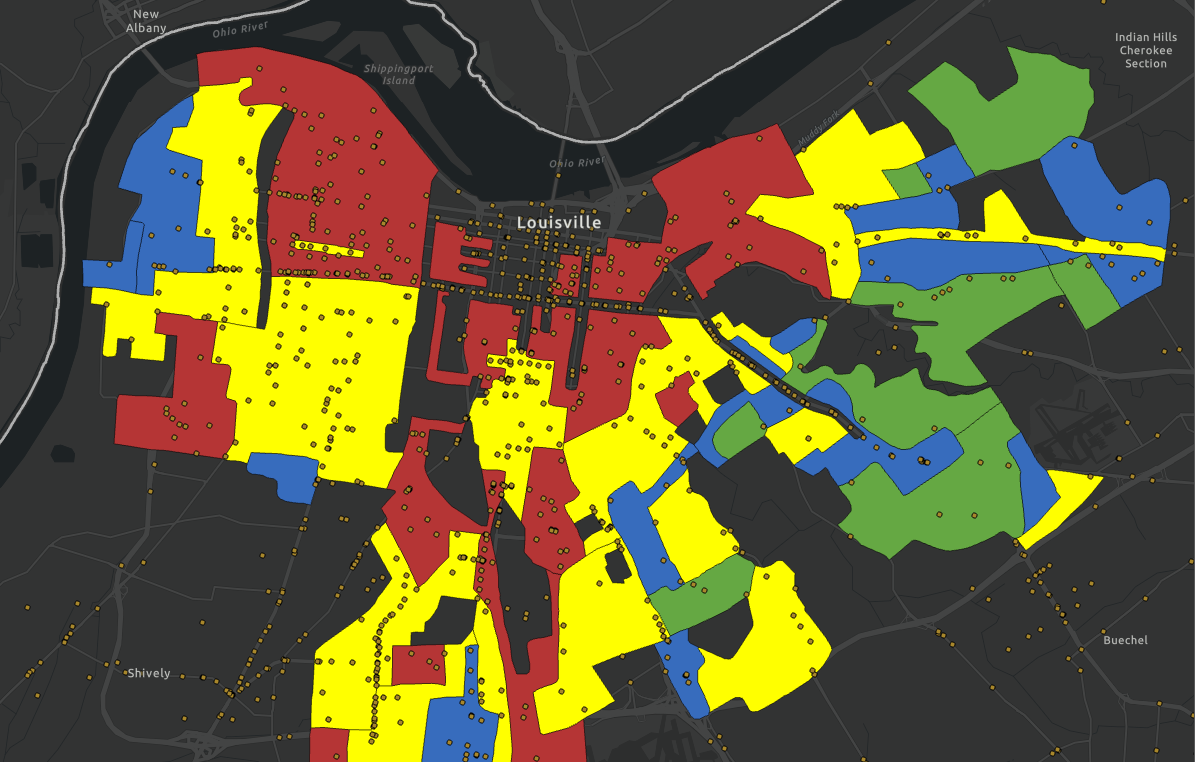
Redlining was a common practice in Louisville from 1933 to 1951. Most of the pre-merger city was assigned a grade by the Home Owners Loan Corporation (HOLC). These grades of A, B, C, or D basically correlated with the presence of minorities in a given area. A grade usually meant the most “safe” areas to give loans (whitest areas) and D grade the least “safe” (highest minority populations). The D grade areas were often depicted as red on maps, hence the term redlining. There was also significant amounts of housing discrimination in the city outside of official redlining, through discriminatory housing covenants, that had similar effects to redlining.
“They are characterized by detrimental influences in a pronounced degree, undesirable population or an infiltration of it. Low percentage of homeownership 1 -very poor maintenance, and often vandalism prevail. Unstable incomes of the people and difficult collections are usually prevalent. The-areas are broader than the so-called slum districts. Some mortgage lenders may refuse to make loans in these neighborhoods and others will lend only on a conservative basis.” - Explanation text from the 1937 HOLC map, referencing D grade areas.
When looking at a map of redlined areas in Louisville, it is obvious that more urban neighborhoods received lower grades while the more suburban ones received higher grades. This reflects the demographics of these areas, even now. The only exception is the Shawnee area, which receives a B grade as it had a higher white population at the time.

Given that these neighborhoods have faced discrimination for so long, and it is reflected in their built environment, it would follow that the dilapidated urban environment could be connected to worse health outcomes. Studies of cities affected by redlining have shown that redlined areas have worse health outcomes.
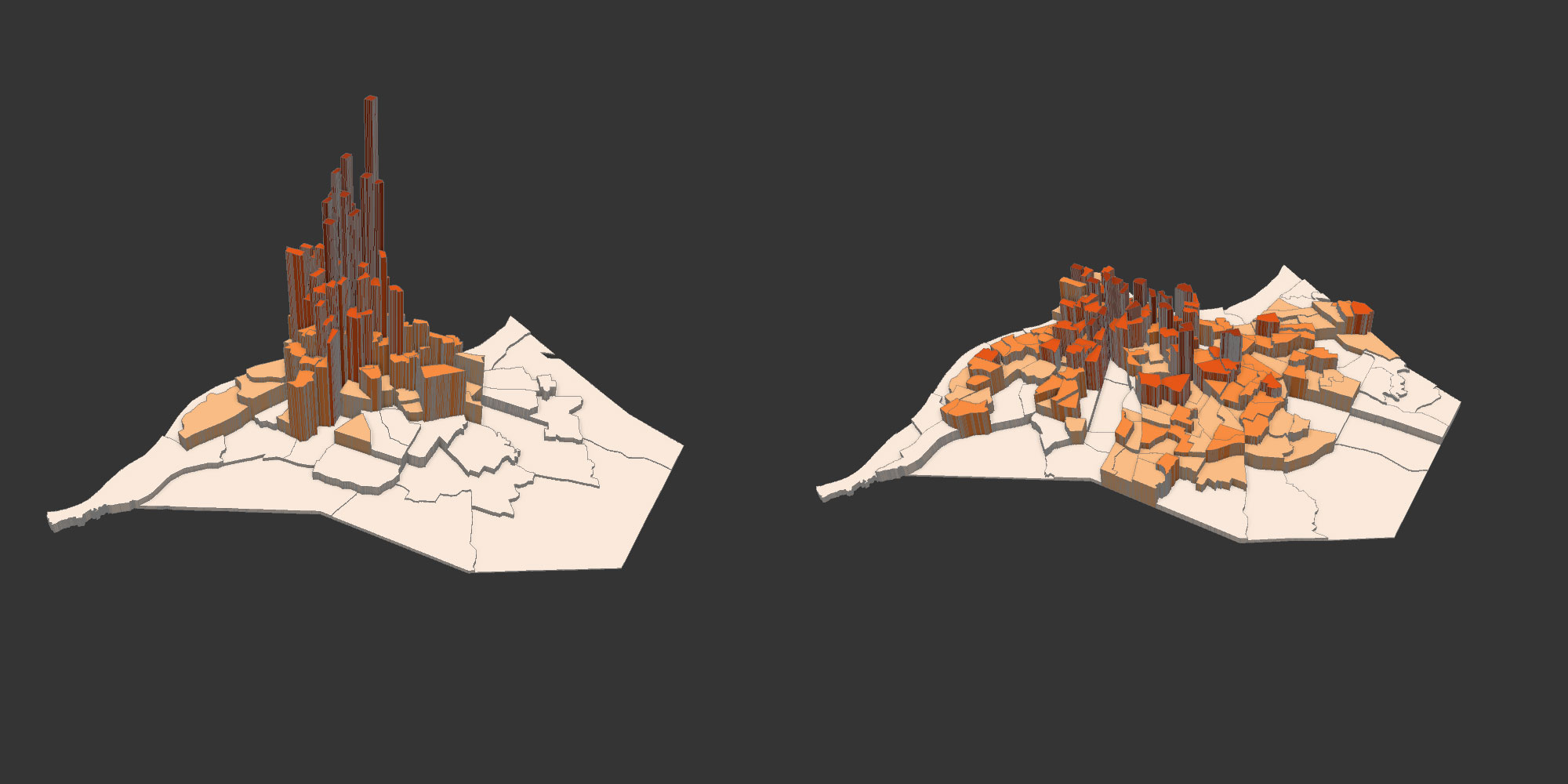
The CDC releases data every year on health outcomes and rates of certain diseases on the census tract level. Using this, we can see what differences we have in health outcomes in Louisville. The one issue that arises with this kind of analysis, though, is that the redlined areas of the 1930s-50s do not align the boundaries of modern day census tracts. In order to gauge the differences in health outcomes, the app below will designate census tracts by their class based on which was most common within the tract. Some tracts that were technically redlined were not included because the redlined area was very small relative to the entire area of the tract. The PLACES data includes hundreds of different possible health conditions, so a handful were selected for readability and generally gauge the difference between these tracts so it is not completely comprehensive. The chart at the bottom shows the average occurrence of the conditions among all tracts of each grade. You can click on tracts to see their individual stats.
Click here to open the interactive map below in its own window
The prevalence of the selected conditions between these census tracts are quite different depending on the grade they were given by the HOLC. With every selected measure, the lower the grade, the worse the health outcome. The difference varied quite a bit, but some of these were large, such as obesity. In the app, the national average prevalence of each condition was also included and that shows that D grade areas were most likely to be above the national average. Despite that, some C and B grade tracts were also above the national average.
These results provide a glimpse into the health dichotomies between redlined neighborhoods and those assigned a higher grade. This does not necessarily paint the full picture, some measures not selected could deviate from this trend, but the selected measures are representative of some of the most common and deadly health afflictions in the country and at least show the juxtaposition between areas with those conditions. A full-fledged study utilizing as much PLACES data as possible would be ideal for determining the differences of health in general between these tracts.